What's a Little "Kink" Amongst Friends? (Part 1)
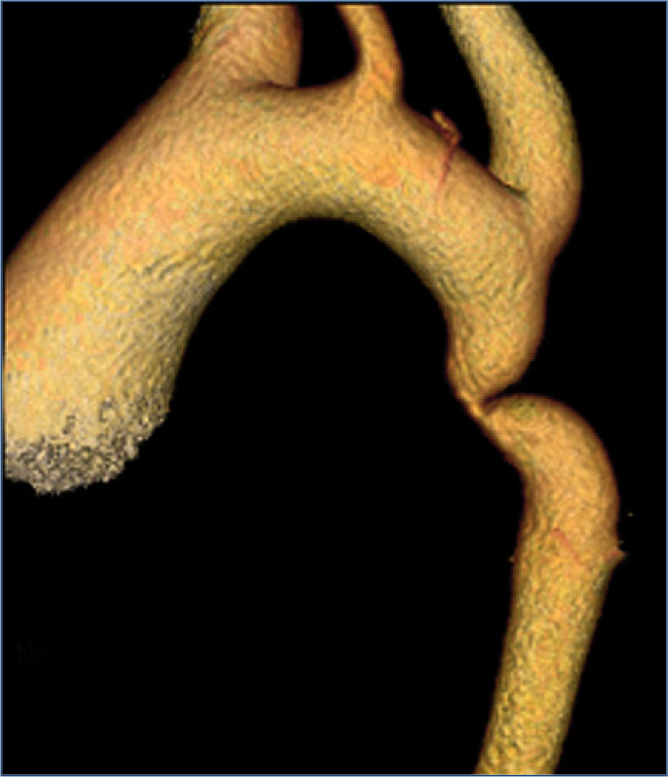
Aortic coarctation is a congenital disorder of the aorta, affects 5% to 8% of all patients with congenital heart disease and is the 7th most common congenital heart disease. During embryologic development, the aorta develops from several primordial structures which coalesce into what we think of as a “normal” aorta. However, sometimes that development process goes awry, resulting in a “kink” or narrowing (stenosis) in the aorta just beyond the left subclavian artery.
Let’s briefly discuss the embryologic basis of aortic coarctation. For those of you who aren’t too interested in the embryology, feel free to jump ahead. In the 3rd week of gestation, there are a series of paired aortic arches. (Adults only have one aortic arch, by the way, which is conventionally a “left-sided” arch for most people.)
It is possible to have a “right-sided aortic arch” or even a double aortic arch without knowing it. For the most part, patients with right-sided and double aortic arches do quite well and don’t have too many problems. Sometimes the double aortic arch can cause swallowing problems, though. The 4th aortic arch persists on the left (which ultimately forms the aortic arch after birth) and the 6th aortic arch develops beyond the 4th segment into the “ductus arteriosus”. The ductus is open at birth and connects the pulmonary artery to the aorta for fetal circulation. The ductus closes naturally several days after birth and as the ductus closes the tissue contracts and can infrequently “kink” or narrow the aorta.
There are a host of associated medical problems which can be associated with aortic coarctation, such as bicuspid aortic valve, arrhythmias, Turner’s syndrome, Sturge-Webber syndrome, Neurofibromatosis and Williams syndrome. Most of the time the coarctation is identified shortly after birth because of a loud heart murmur. When found as an infant, it is usually surgically corrected by cutting out the narrowing and sewing the two ends of the aorta together. If the infant is unstable, a balloon angioplasty can be performed to help the child get better until they can have open surgery.
However, there are a number of infants that don’t have the aortic coarctation identified at birth, and they grow normally. Some patients even make it to adulthood without knowing they have aortic coarctation. The oldest person I have taken care of with an aortic coarctation was 62! Nevertheless, people with untreated coarctations don’t do well.
There is a 90% mortality by age 50 and the average age of death is 35 years of age. The narrowing of the aorta restricts blood flow to the lower extremities. Many people with coarctation complain that they cannot run well because their legs get heavy from lack of circulation and they could never keep up with their classmates in school. In addition, the blood pressure in the upper extremities is greater than in the lower extremities in patients with aortic coarctation because the blood has trouble moving through the restriction in the aorta on the way to the legs.
Aortic coarctation is not something that you can develop later in life. It can also be associated with aortic aneurysms and aortic dissections which complicates the treatment. There are several types of treatment available for aortic coarctation, and we will review them in a future post.
Have you ever heard of this disease before?
Was this post informative?
Subscribe to my newsletter to learn more about the aorta, its diseases, and how to treat them.
Comments
Share your thoughts below — I try to get back to as many comments as possible.