Complete Aortic Blockage (Leriche Syndrome)
Introduction
Yogi Berra, the hall of fame baseball catcher, and master of witty quotes, provided the inspiration for this post. Yogi Berra had a remarkable way with words, and frequently helped us understand life better through his oxymoron-type quote.
If there is a fork in the road, take it.
— Yogi Berra
You may be wondering: “How do Yogi Berra and aortic disease go together?”
This week, I was treating a patient with a complex aortic problem and Yogi Berra’s quote came to mind. I believe the connection with today’s topic and Yogi Berra’s quote will become evident as you keep reading.
Another interesting angle to this post is that we are today’s post expands our understanding of aortic disease beyond aortic aneurysms and aortic dissections because it discusses an utterly different form of aortic disease than we have previously included.
History
Dr. Rene Leriche (1879-1955) was one of the founders of modern vascular surgery. A flamboyant French Surgeon, Dr. Leriche develop a number of different surgical procedures that we still use today. An interesting side note is that the famous French painter, Matisse, was a patient of Dr. Leriche’s.
In addition to developing surgical procedures, his name is linked to an uncommon, but debilitating disease.
Leriche syndrome, also called total abdominal aorto-iliac occlusive disease, refers to a situation when the abdominal aorta and both iliac arteries become completely occluded (blocked).
Anatomy of the aortic bifurcation
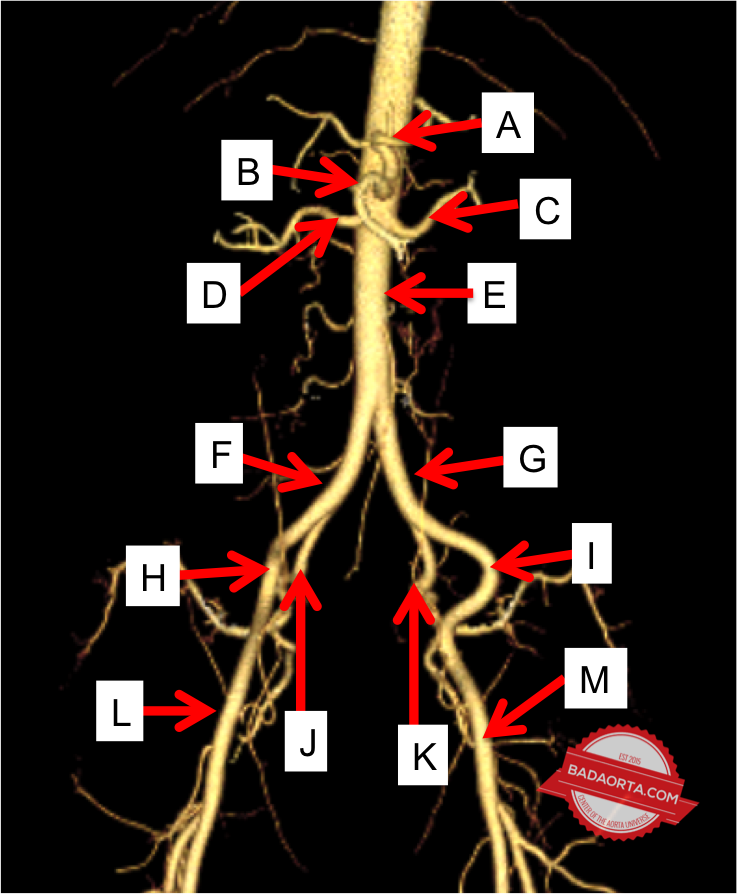
As you recall (refer to my Atlas of Aortic Disease), the aorta runs the length of the torso. At the level of the belly button (navel), the aorta divides into 2 important branches. This bifurcation gives rise to the left and right iliac arteries. This is anatomically the end of the aorta.
Literally (and figuratively as related to Yogi Berra’s quote), this branching point is a “fork in the road”.
The iliac arteries (right and left) provide blood flow to the legs. People are frequently surprised to learn that the blood supply to the legs starts in the lower abdomen. Furthermore, disease, or blockages, in the iliac arteries above the waist can contribute to poor circulation in the feet.
Leriche syndrome
In some people, atherosclerosis (build-up of cholesterol and calcium - sometimes referred to as “plaque”) progresses so significantly that a blood vessel (artery or even the aorta) can become completely blocked.
When this process develops in the lower abdominal aorta, including the aortic bifurcation, the aorta can become completely occluded. What is unique to Leriche Syndrome is that the total blockage develops mostly in one portion of the aorta (aortic bifurcation). Despite this build-up of atherosclerosis in one portion of the arterial tree, the rest of the cardiovascular system often remains unaffected.
Signs and symptoms associated with Leriche syndrome?
Leriche Syndrome is characterized by a triad of buttock and leg claudication (see below), diminished pulses to the feet and impotence.
As a result of the aorta being completely blocked, blood supply to both lower extremities along with the pelvic circulation are affected.
Buttock claudication is a term which describes pain in the hips and upper thighs associated with walking. The aortic bifurcation gives rise to blood vessels that supply the large muscles of the hips such as the gluteus maximus (buttock muscles).
While sitting and at rest, the hip muscles can get enough blood supply through accessory branches off the aorta (called collaterals). However, when someone with Leriche Syndrome begins walking, the hip muscles require increased blood (oxygen).
With the obstruction of the aorta, these muscles cannot obtain enough blood to compensate for the increased need. As a result, and the muscles start cramping due to an excessive build-up lactic acid (anerobic metabolism) and produces a heaviness feeling in the hip muscles.
When the individual stops walking and sits down and rests, the muscles decrease their need for increased blood and the lactic acid washes out. The cramping and heaviness sensation goes away after about 10 minutes and will return the next time they try and walk.
As a result, people with Leriche Syndrome have a limited capacity to walk around.
People with Leriche Syndrome also develop impotence due to a decreased blood supply to the genitals, which is a result of the same process of lack of blood supply to the hip muscles.
The third and last sign of Leriche Syndrome is decreased pulses to both feet. Once again, this occurs equally in both legs due to the aortic bifurcation being completely occluded. The aortic bifurcation gives rise to the arteries to both legs and if this area becomes occluded, then both feet have diminished pulses.
What causes Leriche Syndrome?
Leriche Syndrome usually occurs in younger (40-50 year olds) patients. The overwhelming culprit appears to be tobacco smoking. Most of these patients are heavy smokers and it is incredibly rare to develop in a non-smoker.
Other associated risk factors are high blood pressure (hypertension), elevated blood cholesterol (hypercholesterolemia) and a family history of atherosclerosis.
There are still many things we need to learn about this disease and this is an active area of research.
Diagnosis of Leriche Syndrome
The diagnosis of Leriche Syndrome begins with a discussion with a physician. When someone describes pain in the buttocks/hips with walking (claudication) the physician will check the pulses in both legs and feet.
Next, an abdominal ultrasound is performed which measures blood flow in the abdominal aorta and iliac arteries. Likewise, the circulation is measured in both lower extremities using a test called ankle-brachial index (ABI).
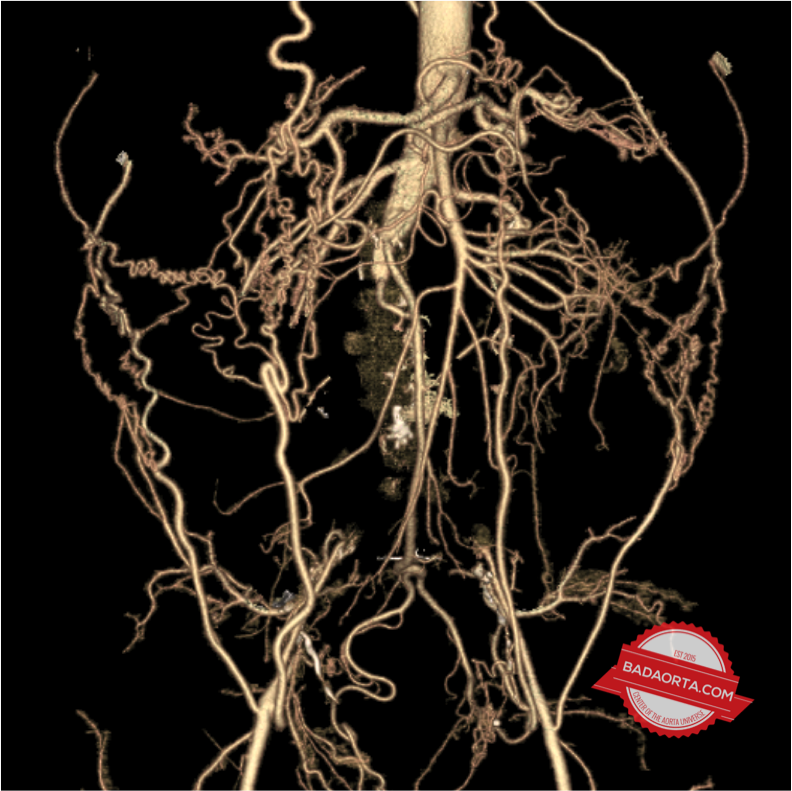
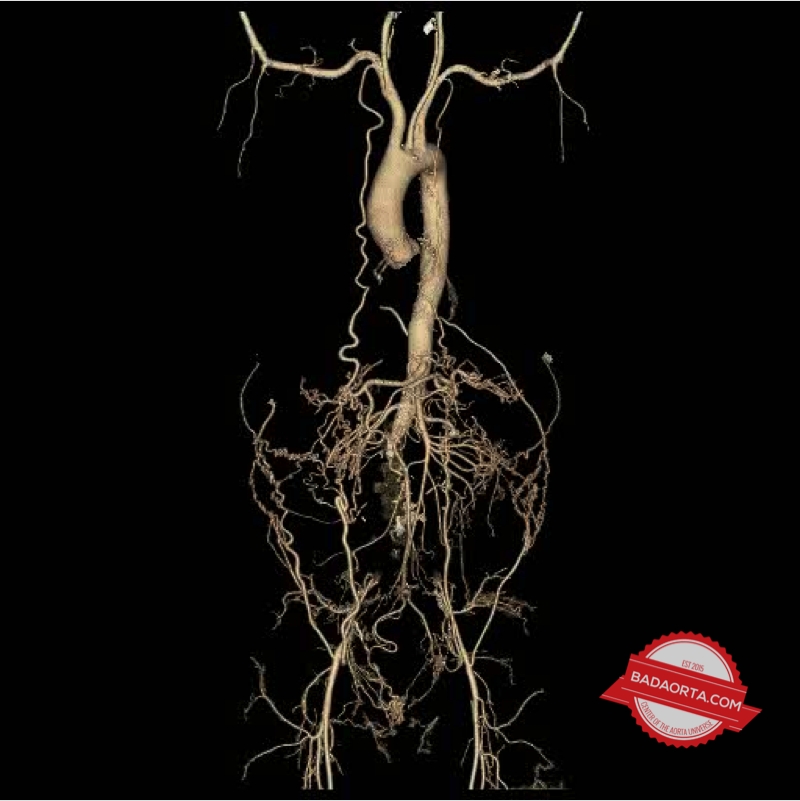
If the abdominal ultrasound test is abnormal, then a CAT scan of the abdomen (with intravenous contrast) is performed. The CAT scan will demonstrate the circulation and demonstrate the obstruction of the lower abdominal aorta and aortic bifurcation.
Collateral blood vessels are also seen as a compensatory mechanism for blood to reach the lower extremities by going around the blockages in the aorta and iliac arteries.
Treatment of Leriche Syndrome
The goal of treating Leriche Syndrome is to restore circulation to the pelvis and both lower extremities.
Unfortunately, there is no medication which can eliminate the blockage. Some medications and blood thinners help maintain the limited circulation.
The two methods of treating Leriche Syndrome are interventional stenting or open aortic surgery.
The traditional method of treating this problem is to create a surgical bypass from the healthy, normal aorta to both common femoral arteries (in the groin region) through an artificial cloth tube with two branches. The blockage is left in place and a new channel for blood flow is created to both lower extremities.
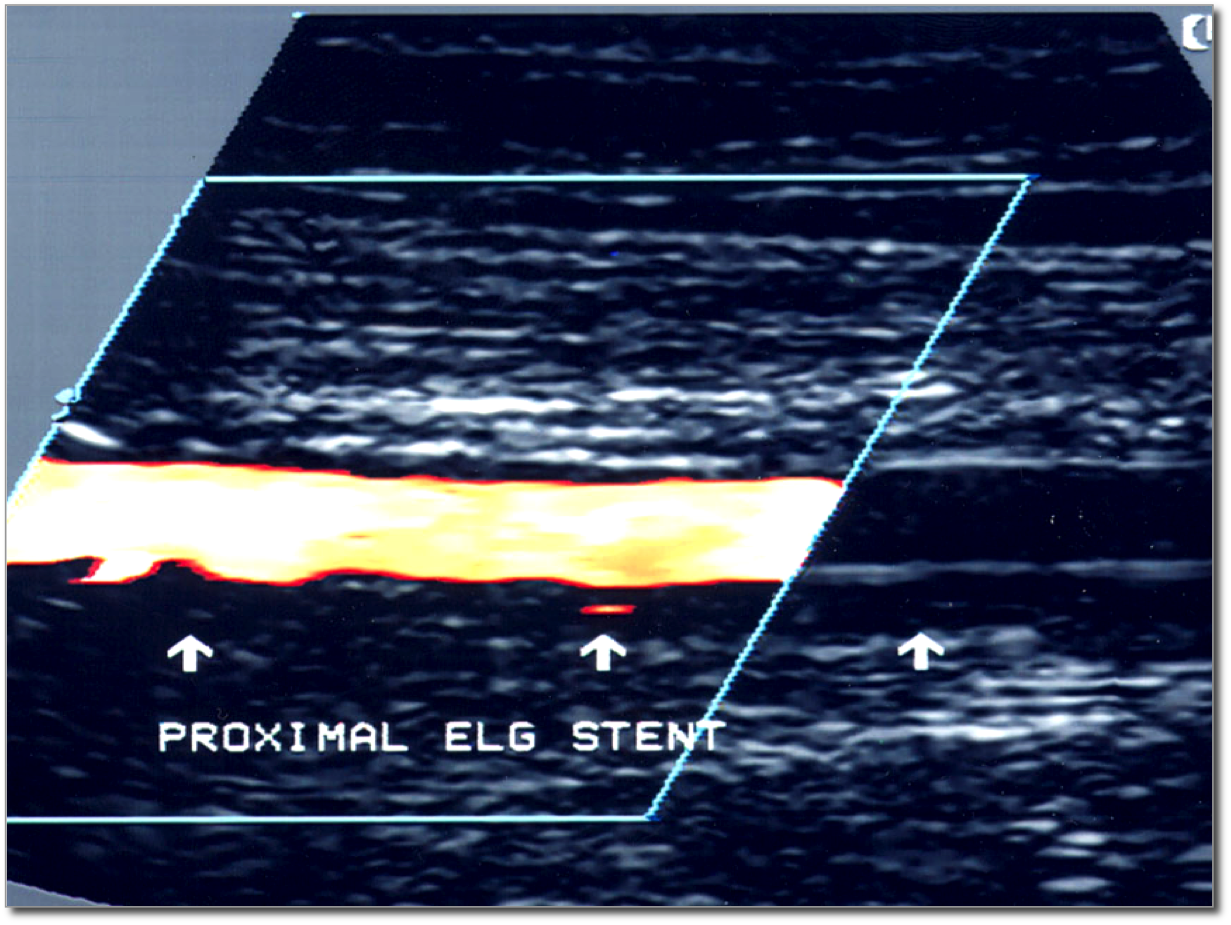
A newer, less-invasive method is to use endovascular techniques to insert stents from both groins into the aorta which sit within the diseased aorta and iliac arteries and create new blood channels within the blockage.
The long-term success of the endovascular option is still being studied. This option is not always available to all patients due to specific anatomic limitations unique to some patients.
At minimum, patients need to stop smoking to prevent further build-up and keep the newly created surgical bypasses or stents open. Medications such as blood pressure medications and statins are also important.
Summary
Leriche syndrome, also called aorto-iliac occlusion, develops from an excessive build-up of plaque (atherosclerosis) in the lower abdominal aorta and aortic bifurcation. Patients with Leriche syndrome present with a triad of buttock muscle pain with walking, impotence and decreased pulses to both feet.
This condition can be treated with either open surgical bypass or newer, less-invasive endovascular stent techniques.
Do you now see the connection between Leriche Syndrome and Yogi Berra?
“If there is a fork in the road, take it.” In aortic terms: “if there is a block in the aortic bifurcation, treat it.”
I think Yogi Berra would be proud.
Questions
What are your thoughts about the different treatment options between open aortic surgery and endovascular stenting?
Share your comments below.
PS. Don’t forget to check out the newly updated Aortic Atlas.
Was this post informative?
Subscribe to my newsletter to learn more about the aorta, its diseases, and how to treat them.
Comments
Share your thoughts below — I try to get back to as many comments as possible.