Hybrid: It's not just for cars, it's also useful in aortic surgery
We all know about those hybrid cars.
When Toyota introduced the Prius in 2008, we all marveled at the exciting new opportunities afforded by the revolutionary concept of seamlessly combining an electric, rechargeable engine with a combustible engine.
Similarly, there are remarkable benefits to patients with aortic disease when we combine endovascular aortic stenting with conventional open aortic surgery.
Voila! Thus the concept of hybrid aortic procedures is born.
Differences between endovascular and open aortic procedures

Less-invasive endovascular aortic stenting procedures (EVAR or TEVAR) do not involve opening the chest or abdomen. Instead, the compressed aortic stents are inserted into the body through a small incision in the groin and advanced within the body using Xray guidance (fluoroscopy).
When the aortic stent is positioned correctly within the aneurysm, it is released and instantly begins working.
On the other hand, open aortic surgery involves a large incision in the chest or abdomen. Through this large incision, adjacent organs such as the lungs, heart, or intestines are pushed aside and the aneurysm is cut-out. A synthetic polyester tube is then sewn in place to replace the removed aneurysm.
The differences between these procedures are dramatic.
With a smaller incision, the endovascular procedures allow for quicker recovery to normal activity with less pain along the way.
However, some aneurysms are located in portions of the aorta that are even more challenging to repair.

Aneurysms located in the aortic arch or in the upper abdomen (called the thoracoabdominal aorta) involve major branches of the aorta to vital organs.
Blood flow to the head and brain originates from the aortic arch. Blood flow to the kidneys, intestines and vital organs originate from the thoracoabdominal aorta.
Aortic stents with branches are (for the most part) still research devices and the current generation of aortic stents on the market don’t have the ability to accommodate blood flow to branches of the aorta supplying vital organs.
Hybrid aortic procedures
For patients with complex aortic aneurysms involving the aortic arch and abdominal aorta, we can combine the benefits of endovascular aortic stenting with open aortic surgery to decrease the overall impact of the aortic repair on the patient.
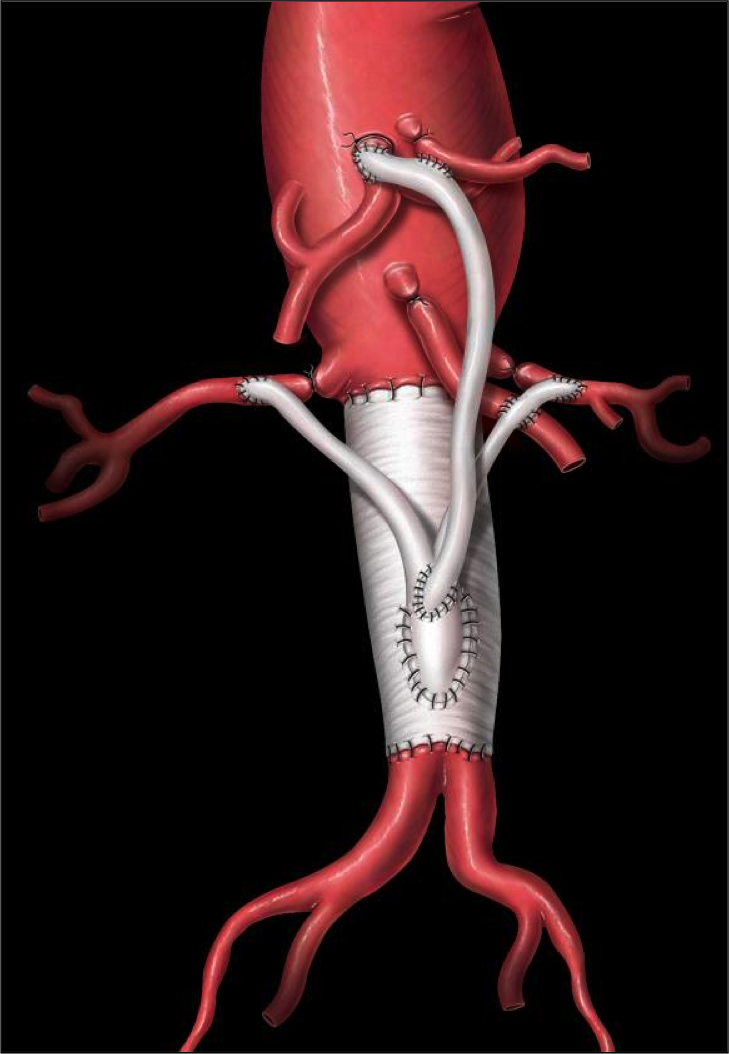
For example, with an aneurysm in the aortic arch - through the same incision used for open aortic surgery - we can create bypasses of the great vessels which maintain blood supply to the brain.
Once these branches are bypassed, we can treat the aortic arch with an endovascular stent. The combined insult to the patient is less than a standard aortic arch replacement with circulatory arrest.
Similarly, an open abdominal incision with bypasses to the renal and visceral arteries followed by an aortic stent from the thoracic aorta all the way to the aortic bifurcation is less invasive than a thoracoabdominal incision and aortic replacement.
1 + 1 = 3
What we have done with these hybrid aortic procedures is combine the best of open aortic surgery with the best of endovascular procedures. At that nexus, or interface between the procedures, new treatment options become available.
These hybrid procedures also involve unique skills on behalf of the surgeon. In order to perform these types of procedures, surgeons need to be proficient in both open aortic surgery and endovascular procedures.
Additionally, these procedure need to be performed in specially-equipped operating rooms, called hybrid ORs. Most open heart surgery operating rooms don’t have the special Xray imaging equipment. Likewise, most Xray equipped operating rooms don’t have the necessary open heart surgery equipment.
As you can appreciate, these specialized hybrid aortic procedures are highly intricate and require special skills and equipment.
Comparison with standard open aortic surgery
Hybrid aortic procedures are relatively new procedures. As such, we don’t have long-term follow-up data for these procedures.
However, we do have several publications which have compared the early-term results versus standard aortic surgery and the two are at least comparable. There are no significant differences between the two types of procedures. This is something that will still need to be studied and followed.
Conclusion
In conclusion, the exciting opportunities afforded by endovascular aortic stents has also contributed to changing and improving standard aortic surgery.
Was this post informative?
Subscribe to my newsletter to learn more about the aorta, its diseases, and how to treat them.
Comments
Share your thoughts below — I try to get back to as many comments as possible.