Image(ing) Is Everything
In every presentation that I give - whether it is in the United States or internationally - there is a common theme that I emphasize with the audience.
The theme is: With regards to treatment of aortic diseases such as aortic aneurysms or aortic dissections, “Imaging is Everything”.
What do I mean by that?
When a patient is diagnosed with an aortic problem, such as an aortic aneurysm, the first thing we do is review the diagnostic imaging studies (chest X-rays, CT scan or MRI).
With advanced imaging, we are able to see the aorta in new and different ways.
Here is a 3D reconstruction of a CT scan of the aorta.
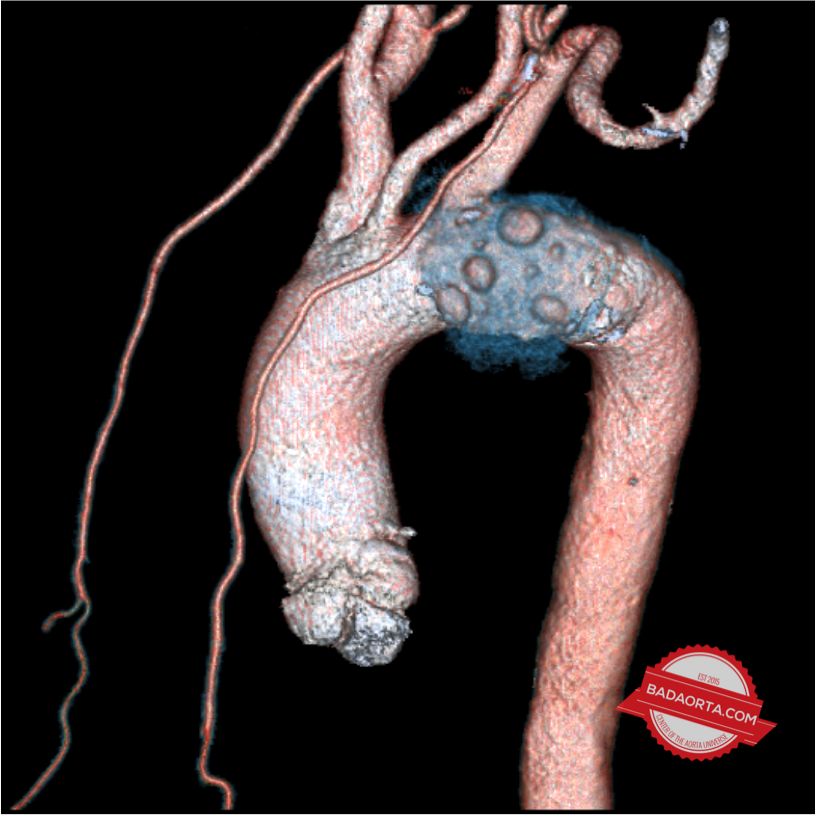
The value of this imaging study and data is that we can see the aorta in ways that we previously couldn’t.
By seeing the aorta from new perspectives, we can envision and plan for new ways to treat the aorta. Those treatments could be open surgery, endovascular aortic stents or hybrid procedures which combine the best of open surgery with the best of endovascular procedures.
The first teaching point here is that case planning for aortic procedures is extremely important. When we are planning for a patient’s surgery there are a lot of details which are all driven by the patient’s unique anatomy.
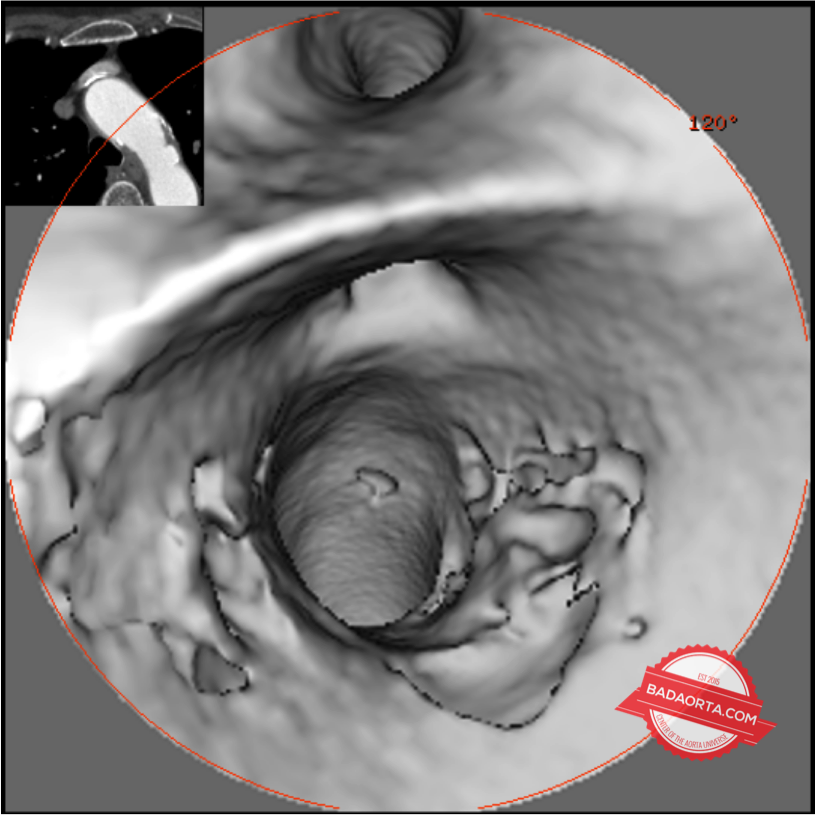
In addition to 3D reconstructions, we can use the same data obtained from standard CT scan to reconstruct the inside of the aorta. The beauty of this technique is that it does not involve specialized equipment and the imaging data is essentially captured on almost all high resolution CT scans performed currently.
The CT scan imaging data is then reconstructed to provide internal views of the aorta that we have never seen before.
Another imaging modality that we rely on is intravascular ultrasound, also called IVUS. IVUS is a very important adjunct to our aortic case planning.
It is an invasive technology and involves inserting a small catheter, with a transducer at the end of the catheter, inside the aorta. The vascular access point for the entry is usually the femoral artery in the groin and using X-ray guidance, we can navigate the catheter and probe into position inside the aorta.
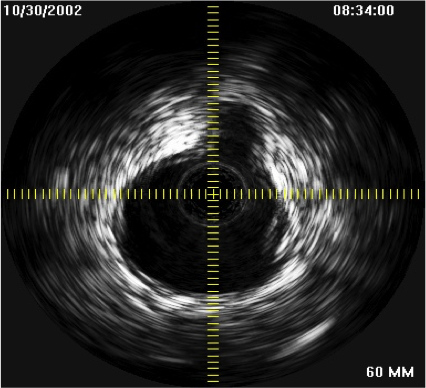
The transducer at the end of the catheter emits ultrasound waves which penetrate the surrounding tissues without causing damage. The waves are then reflected back depending on the types of tissues and quality of tissues that surround it.
IVUS is simple to use but is infrequently used by clinicians because it is unfamiliar to many of them. We are trying to get the word out about the value of this imaging modality for patients and physicians.
As you can see, as we can visualize more of the aorta, we can have better information in which to base our treatment decisions.
Thus, as the imaging gets better, our treatments get better and as our treatments get better, our imaging gets better. It is a positive feedback loop.
For more information about the imaging check out my other website: drgraysonwheatley.com
Was this post informative?
Subscribe to my newsletter to learn more about the aorta, its diseases, and how to treat them.
Comments
Share your thoughts below — I try to get back to as many comments as possible.