Stenting the Ascending Aorta
Stenting of the Ascending Aorta
Other than open surgical repair of the proximal aorta (aortic root and ascending aorta) for aortic aneurysms and aortic dissections, one of my main professional interests is stenting of the ascending aorta.
This is what an acute Type A aortic dissection looks like:
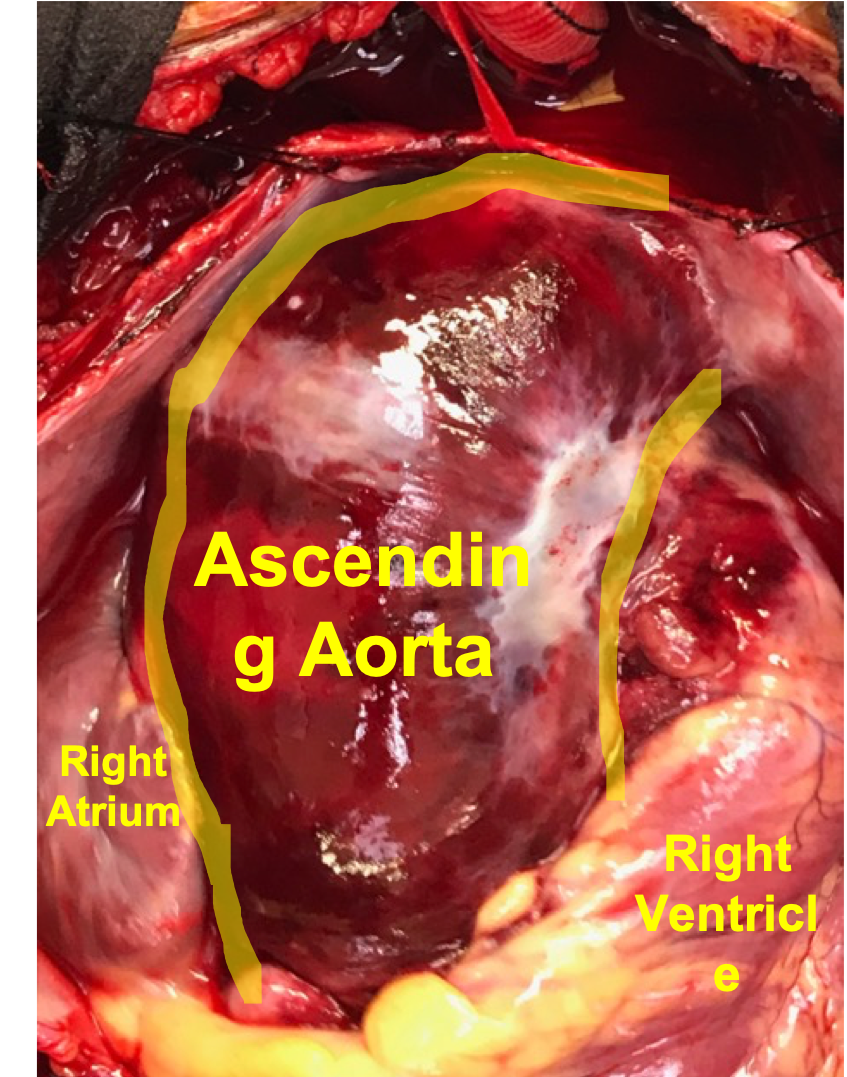
Acute Type A aortic dissections are an emergency and need to be treated. This image demonstrates (from the outside of the aorta) how irritated and traumatized the ascending aorta looks shortly following onset of an acute Type A aortic dissection.
Stenting of the ascending aorta is a nascent field, with limited information and a deficit of a codified set of rules or guidelines.
Few physicians, surgeons or hospitals have much experience with endovascular repair of the ascending aorta (or are even familiar with it).
I am fortunate to be a part of a small group of physicians globally who are helping champion and develop this less-invasive approach to the ascending aorta.
Over the last 10 years, I have treated a significant number of patients who have had a wide range of ascending aortic problems utilizing stents in the ascending aorta. I have one of the largest experiences with endovascular repair of the ascending aorta.
A number of patients from across the country have reached out to me directly through my website and have inquired about whether they could be a candidate for ascending aortic stenting.
Therefore, I wanted to provide a summary and overview of endovascular repair of the ascending aorta for patients and physicians looking for more information.
[If you or a family member are interested in learning more about stenting of the ascending aorta, or to inquire about your specific medical condition, email info@badaorta.com, fill out a contact form or call my office 615-342-6900. I will speak with you directly, and then have you send me your medical records and your CAT scans. Once I receive the medical records and CAT scans, I will call you back to discuss my impressions. If a surgical or endovascular procedure is appropriate, my office will then help you coordinate a trip to Nashville to be treated.]
Wheatley’s Aortic Rule #1
As with all aortic-related problems, we must start with Wheatley’s Aortic Rule #1.
You must understand the anatomy of the aorta before you can understand the treatment.
Aortic diseases can be quite complex and nuanced, so it is critical to develop an introductory knowledge of aortic anatomy.
The ascending aorta is particularly subtle and complex area which that translates into a very complex process surrounding the endovascular treatment of the ascending aorta.
The aorta, being the main blood vessel of the body, literally connects to the heart at the level of the aortic valve. The aortic valve is the regulator between blood inside the left ventricle of the heart and the aorta.
Every beat of the heart enables the heart muscle to quickly fill with blood which is then ejected in a coordinated fashion with each contraction of the heart muscle.
Blood which is ejected from within the left ventricle of the heart exits the heart by passing through the aortic valve and immediately enters the aortic root.
The aortic root is a very compact area with a great deal of anatomic features concentrated together.
The aortic valve leaflets, when open, extend up into the aortic root. Most people think of the valve leaflets opening and closing within a single plane, but in fact, the leaflets reach upwards above the aortic valve annulus (place of attachment of the leaflets and the physical ) for a distance of 1.5 centimeters.
The aortic root has a natural bowing-out of the aortic wall (called sinuses) and is not a straight tube in this section as you might think. These outpouchings allow the aortic valve leaflets to fully open and still maintain blood behind the leaflets for filling the coronary arteries.
The coronary arteries - which provide blood flow to the heart muscle - originate from within the aortic root a short distance above the aortic valve annulus.
There are two main coronary arteries (one for each side of the heart - left and right).
It is a paradox that the heart muscle is full of blood and that blood does not nourish the heart muscle. For the heart muscle to receive nourishing blood, the blood must exit the heart, enter the left and right main coronary arteries and then travel “backwards” on the external surface of the heart. The arcade of arteries on the outside of the heart muscle continuously branch and create a network of channels which provide oxygenated blood to each muscle fiber of the heart.
At the top of the aortic root is the sinotubuar junction. The distance from the aortic annulus where the aorta attaches to the heart to the sinotubular junction is approximately 2 cm.
This area represents the formal anatomic transition from the outpouchings of the aortic root (sinuses) with the circular and straight portion of the ascending aorta.
The ascending aorta is appropriately named because the heart sits in the middle of the chest and the aorta literally “ascends” up the middle of the chest behind the breast bone (sternum). At the base of the neck, the aorta starts curving around to become the aortic arch.
The aortic arch represents the transition from the ascending aorta to the descending aorta. It also provides blood flow to the brain and upper arms through branches.
Unique Features of the Ascending Aorta
The ascending aorta, besides being composed of two distinct parts (aortic root and ascending aorta proper), is quite compact.
The ascending aorta is relatively short. The distance from the sinotubular junction to the aortic arch ranges from 4 to 10 centimeters. [Remember those numbers,,,]
In addition, the ascending aorta is curved. The angle at which the ascending aorta connects to the heart varies from person to person. Sometimes it is vertical and sometimes horizontal and everything in between. This angularity creates a gentle curve for the ascending aorta to transition into the aortic arch.
There is a lot of motion and movement to the ascending aorta. The cardiac output from the heart represents a violent ejection of pressurized blood being released from the heart. The ascending aorta is the “shock-absorber” which accepts the cardiac output in full force. This causes more motion compared to the descending thoracic aorta.
The violent expansion and contraction of the ascending aorta creates more stress to the elastic tissues of the aortic root and ascending aorta.
The repeated stress to the aortic wall in the aortic root makes this area more susceptible to rips and tears of the aorta (called aortic dissections) than other parts of the aorta.
We will discuss ascending aortic stenting in more detail with additional articles on this site.
Was this post informative?
Subscribe to my newsletter to learn more about the aorta, its diseases, and how to treat them.
Comments
Share your thoughts below — I try to get back to as many comments as possible.